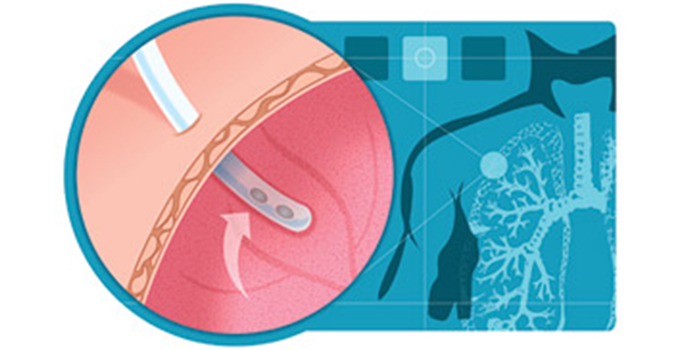
There are many clinical conditions that may necessitate the use of chest tubes. When there is an accumulation of positive pressure in the chest cavity (where it should normally be negative pressure between pleurae), a patient will require chest drainage. Chest tubes may be inserted to drain body fluids or to facilitate the re-expansion of a lung. No matter what the reason or underlying cause, chest tubes help to resolve the problems associated with large volumes of air or fluid that have collected in the pleural space. When air or fluid enters the pleural space, the lung cannot expand properly. In some cases, chest tubes can also be used for certain therapy-related patient management as well. The use of chest tubes is not completely fail safe; complications can arise.
Indications for Chest Tubes (Chest Drainage Systems)
There are various reasons for excess air and/or fluid in the pleural space. Specific common indications for chest tubes include:
- Pneumothorax (open and closed).
- Tension pneumothorax.
- Hemothorax.
- Hemopneumothorax.
- Pleural effusions.
- Chylothorax (a type of pleural effusion that results from lymphatic fluid (chyle) accumulating in the pleural cavity).
- Penetrating chest trauma.
- Pleural empyema (collection of purulent material in the lungs).
(Durai, Hoque, & Davies, 2010) - Excess air and/or fluid accumulation in the pleural space. For example, chest tubes are often placed after cardiac surgery to drain blood associated with the surgery (Doelken, 2010).
- Need for pleurodesis: Pleurodesis is a procedure used to treat patients with recurrent pleural effusions or recurrent pneumothorax. This procedure involves administering a sclerosing agent into the pleural space which causes the visceral and parietal pleura to adhere to each other without the thin coating of fluid between them. Chemical pleurodesis is a painful procedure, and patients are often pre-medicated with a sedative and analgesics. A local anesthetic may be instilled into the pleural space, or an epidural catheter may be placed for anesthesia.
- Chemotherapy administration: May be administered through a chest tube.
- Trauma
- Lung disorders
- Factors that compromise pulmonary function (e.g. COPD, smoking)
- Invasive pulmonary procedures (bronchoscopy)
- Cardiopulmonary resuscitation
- Surgical complication
- Complications from central line insertion v
- Mechanical ventilation using positive end-expiratory pressure
- Purulent substances from an infection
- Any underlying clinical condition that results in excessive air/fluid in the pleural space (eg. pulmonary embolism and cancer)
Other indications include:
Causes of Injury to the Chest Wall
The causes of the indications previously mentioned collectively include:
CLICK HERE for more resources on Fundamentals of Nursing
CLICK HERE for more resources on Laboratory & Diagnostic Test
NURSING INTERVENTIONS
- If using a chest drainage system with a water seal, fill the water seal chamber with sterile water to the level specified by the manufacturer.
- When using suction in chest drainage systems with a water seal, fill the suction control chamber with sterile water to the 20-cm level or as prescribed. In systems without a water seal, set the regulator dial at the appropriate suction level.
- Attach the drainage catheter exiting the thoracic cavity to the tubing coming from the collection chamber. Tape securely with adhesive tape.
- If suction is used, connect the suction control chamber tubing to the suction unit. If using a wet suction system, turn on the suction unit and increase pressure until slow but steady bubbling appears in the suction control chamber. If using a chest drainage system with a dry suction control chamber, turn the regulator dial to 20 cm H2O.
- Mark the drainage from the collection chamber with tape on the outside of the drainage unit. Mark hourly/daily increments (date and time) at the drainage level.
- Ensure that the drainage tubing does not kink, loop, or interfere with the patient’s movements.
- Encourage the patient to assume a comfortable position with good body alignment. With the lateral position, make sure that the patient’s body does not compress the tubing. The patient should be turned and repositioned every 1.5 to 2 hours. Provide adequate analgesia.
- Assist the patient with range-of-motion exercises for the affected arm and shoulder several times daily. Provide adequate analgesia.
- Gently “milk” the tubing in the direction of the drainage chamber as needed.
- Make sure there is fluctuation (“tidaling”) of the fluid level in the water seal chamber (in wet systems), or check the air leak indicator for leaks (in dry systems with a one-way valve). Note: Fluid fluctuations in the water seal chamber or air leak indicator area will stop when:
- The lung has reexpanded
- The tubing is obstructed by blood clots, fibrin, or kinks
- A loop of tubing hangs below the rest of the tubing
- Suction motor or wall suction is not working properly
- With a dry system, assess for the presence of the indicator (bellows or float device) when setting the regulator dial to the desired level of suction.
- Observe for air leaks in the drainage system; they are indicated by constant bubbling in the water seal chamber, or by the air leak indicator in dry systems with a one-way valve. Also assess the chest tube system for correctable external leaks. Notify the physician immediately of excessive bubbling in the water seal chamber not due to external leaks.
- When turning down the dry suction, depress the manual high negativity vent, and assess for a rise in the water level of the water seal chamber.
- Observe and immediately report rapid and shallow breathing, cyanosis, pressure in the chest, subcutaneous emphysema, symptoms of hemorrhage, or significant changes in vital signs.
- Encourage the patient to breathe deeply and cough at frequent intervals. Provide adequate analgesia. If needed, request an order for patient-controlled analgesia. Also teach the patient how to perform incentive spirometry.
- If the patient is lying on a stretcher and must be transported to another area, place the drainage system below the chest level. If the tubing disconnects, cut off the contaminated tips of the chest tube and tubing, insert a sterile connector in the cut ends, and reattach to the drainage system. Do not clamp the chest tube during transport.
- When assisting in the chest tube’s removal, instruct the patient to perform a gentle Valsalva maneuver or to breathe quietly. The chest tube is then clamped and quickly removed. Simultaneously, a small bandage is applied and made airtight with petrolatum gauze covered by a 4 ×4-inch gauze pad and thoroughly covered and sealed with nonporous tape.
CLICK HERE for more resources on Fundamentals of Nursing
CLICK HERE for more resources on Laboratory & Diagnostic Test