Bone Marrow Aspiration and Biopsy
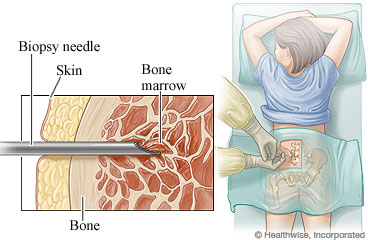
Bone marrow aspiration is one of the diagnostic tools used to assess the status of the hematopoietic system. It involves extracting small amounts of myeloid tissue from a bony cavity (e.g., the sternum or iliac crest). The posterior-superior spine portion of the iliac crest is considered the first choice site because there is a higher percentage of success in obtaining quantities of bone marrow sufficient for diagnostic testing.
Bone marrow aspiration provides accurate information on the relative number of stem cells and their development and morphological structure. A follow-up technique, bone marrow biopsy, provides a more specific morphology of the bone.
OVERVIEW
Complications
● Potentially painful
● Potential hemorrhage at the site
● Risk of introducing infection to the bone, which can lead to osteomyelitis
● Retroperitoneal hemorrhage caused by penetration into the bowel cavity by too deep a penetration of the iliac crest
● Unsuccessful biopsy (known as dry tap)
CLICK HERE for more resources on Fundamentals of Nursing
OPTIONS
● Bone marrow aspiration
● Bone marrow biopsy
RATIONALE
● To assess the hematopoietic system
● To evaluate hematopoietic abnormalities
INDICATIONS
● Unexplained anemia
● Unresolved neutropenia after withdrawal from antibiotic therapy
● Suspected metastatic disease
● Abnormal hematopoietic disorder (leukemia, idiopathic thrombocytopenia, pancytopenia)
● Lymphoproliferative disorders, including lymphoma
● Immunodeficiency disorders, including HIV
● Fever of unknown etiology
● Suspected unusual presentation of an infectious disorder (fungal, tuberculosis)
● Chromosomal analysis
● Bone marrow transplantation
CONTRAINDICATIONS
● Severe osteoporosis
● Hemophilia
● Known radiation to bone site
◗ Informed consent required
PROCEDURE
Bone Marrow Aspiration and Biopsy
Equipment
Prepackaged disposable kits are available.
● Gloves—sterile
● Povidone-iodine (Betadine)
● Fenestrated drape—sterile
● 3-mL syringe
● Two needles—21 gauge and 25 gauge, 1½ inch
● 1% or 2% lidocaine without epinephrine
● 10-mL syringe prepared with ethylenediamine tetra-acetic acid (EDTA) solution
rinse
● Complete blood count purple-top (EDTA) laboratory test tube
● No. 11 scalpel
● Bone marrow aspiration needle
● Jamshidi bone marrow biopsy needles (optional)
● Microscope glass slides
● Fixative specimen container
● 4 × 4 gauze—sterile
● Tape
CLICK HERE for more resources on Laboratory & Diagnostic Test
Procedure
BONE MARROW ASPIRATION—ILIAC CREST
● Position the client comfortably on abdomen. A pillow under the area of the procedure may relax the individual.
● Identify the posterior-superior landmarks.
● Cleanse the area of the aspiration and 3 inches surrounding with povidone-iodine.
● Open the bone marrow kit.
● Put on sterile gloves.
● Draw up lidocaine in the 3-mL syringe with the 25-gauge needle.
● Insert the needle intradermally at the site, and inject a small amount of lidocaine until a wheal has formed.
● Replace the 25-gauge needle with the 21-gauge needle, and penetrate deeper into the tissue until the periosteum of the site is felt. Inject approximately 1 mL into the area; then slowly withdraw while infiltrating the needle tract with the remaining solution.
● While waiting for local anesthetic to work (5 to 10 minutes), confirm that the obdurator of the biopsy needle is locked in place and the cap is secured.
● When the skin is anesthetized, use the No. 11 scalpel and make a small (0.25 cm or less) stab wound.
● Insert the biopsy needle at a 90-degree angle into the incision with the capped end in the palm of hand and the shaft between two fingers (usually index and middle fingers) until resistance of the periosteum is felt.
● Instruct the client that the next part of the procedure may cause a pressure sensation.
● Simultaneously begin to apply downward pressure and alternate clockwise and counterclockwise motions to penetrate the cortex of the bone.
● Continue this until penetration for approximately 1 cm until the “give” of the cortex is felt. Halt downward pressure, and advance approximately 1 to 2 mm farther to ensure placement in the marrow. The biopsy needle should be held in place by the skin and bone.
● Unlock the cap of the syringe, withdraw the obturator, and attach the EDTA-prepared 10-mL syringe.
● Counsel client that pain may be felt at this time and to remain as still as possible.
● Pull up on the plunger of syringe. This creates a vacuum, allowing bone marrow contents to be aspirated. If no material is withdrawn, advance the needle an additional 1 to 2 mm, and repeat aspiration.
● If still no response, withdraw the needle from that periosteum site, and try another site within the incision.
● Withdraw a minimum of 5 mL of marrow. A good specimen shows grossly visible bone spicules.
● Prepare the smears (may be performed by nonsterile assistant) in the following manner – Thinly spread the bone marrow aspiration material over one glass specimen slide and cover with second slide.
● Gently squeeze the two slides together, and allow any excess blood to drain off the slides.
● After excess blood is removed, roll the slides apart lengthwise.
• This allows thinning of any layering of the specimen.
● On successful aspiration, remove the needle, and apply pressure over the area using a quarter-folded 4 × 4 gauze and tape as a pressure dressing.
● Have the client remain supine for 1 hour with pressure dressing in place.
● After 1 hour, the client may get up and leave.
BONE MARROW BIOPSY—USUALLY PERFORMED ON THE ILIAC CREST
● Position the client comfortably on abdomen. A pillow under the area of the procedure may relax the individual.
● Identify the posterior-superior landmarks.
● Cleanse the area of the aspiration and 3 inches surrounding with povidone-iodine.
● Open the bone marrow kit.
● Put on sterile gloves.
● Draw up lidocaine in the 3-mL syringe with the 25-gauge needle.
● Insert the needle intradermally at the site and inject a small amount of lidocaine until a wheal has formed.
● Replace the 25-gauge needle with the 21-gauge needle, and penetrate deeper into the tissue until the periosteum of the site is felt. Inject approximately 1 mL into the area; then slowly withdraw while infiltrating the needle tract with the remaining solution.
● While waiting for local anesthesia to work (5 to 10 minutes), confirm that the obdurator of the biopsy needle is locked in place and cap is secured.
● When the skin is anesthetized, use the No. 11 scalpel and make a small (0.25 cm or less) stab wound.
● Insert the biopsy needle at a 90-degree angle into the incision with the capped end in the palm of hand and the shaft between two fingers (usually index and middle fingers) until resistance of the periosteum is felt.
● Instruct patient that he or she may feel pain and pressure.
● Simultaneously begin to apply downward pressure and alternate clockwise and counterclockwise motions to penetrate the cortex of the bone.
● Continue this until penetration for approximately 1 cm until the “give” of the cortex is felt. Halt downward pressure, and advance approximately 1 to 2 mm farther to ensure placement in the marrow. The biopsy needle should be held in place by the skin and bone.
● When the biopsy syringe has been placed in the marrow, withdraw the needle 3 mm to have it placed in the cortex.
● Redirect the angle of the needle toward the anterior iliac spine, and advance it into the cortex until resistance decreases.
● Remove the obdurator and perform an alternate clockwise and counterclockwise motion for a distance of 2 cm.
● Proceed to rock the needle clockwise five times and then counterclockwise five times to ensure a good specimen.
● Change the angle approximately 15 degrees, and repeat previous step. This allows the specimen to be severed from the marrow.
● Cover the opening of bone marrow needle with your thumb and withdraw it.
● Insert the obturator and allow the specimen to be pushed out onto sterile 4 × 4 gauze.
● Prepare the smears (may be performed by nonsterile assistant) in the following manner
● Using a light touch, gently touch four glass slides to the specimen on the gauze.
● Place the specimen in a container with the fixative agent.
● On completion, remove needle, and apply pressure over the area using a quarter-folded sterile 4 × 4 gauze and tape as a pressure dressing.
● Have the client remain supine for 1 hour with pressure dressing in place.
● After 1 hour, client may get up and leave.
Client Instructions
● Infection rarely is associated with this procedure. Observe for signs and symptoms of infection, however, such as
● Increased redness and warmth at the site
● Red streaks
● Swelling with drainage
● Pus from site
● Contact your health-care provider if any of the following symptoms occur within 48 hours
● Fever
● Abdominal pain
● Unrelieved site pain
● Leave the pressure dressing on for 12 hours. After that time, the dressing may be removed and a standard dressing applied.
● Keep the site clean and dry for 24 hours.
● Avoid strenuous exercise for 48 hours.
● Pain is usually minimal and may be relieved with acetaminophen (Tylenol) or acetaminophen with codeine (Tylenol No. 3).
● Return to the office in 48 hours for recheck.
BIBLIOGRAPHY
McCance K, Huether S. Pathophysiology: The Biological Basis for Disease in Adults and
Children. St. Louis, MO: Mosby; 1996.
Paulman P. Marrow sampling. Am Fam Physician. 1989;40(6):85–87.
Pfenninger JL, Fowler GC. Procedures for Primary Care Physicians. St. Louis, MO: Mosby; 2011.
CLICK HERE for more resources on Laboratory & Diagnostic Test